


🦠 COVID-19 | Re-opening fears and inequity beyond policy decisions

I am a scientist by education, banker at JPMorgan for a few years, then mature PhD student in Chemical Biology at Oxford under the supervision of Christofer Schofield (FRS) and Peter Ratcliffe (Nobel laureate in medicine in 2019). Founder and tech investor focusing on media and education. I care about science, learning and Democracy which are good bedfellows.
📊 Daily Data Brief:
3,812,912 (+87,137) cumulative cases
Active cases: 2,256,618 (+30,801) (this is the number of currently infected patients)
Total Deaths: 264,177 (+5,906)
Serious/Critical Cases: 48,201 (-1,048)
Recovered: 1,292,117 (+50,430)
Source: Worldometers
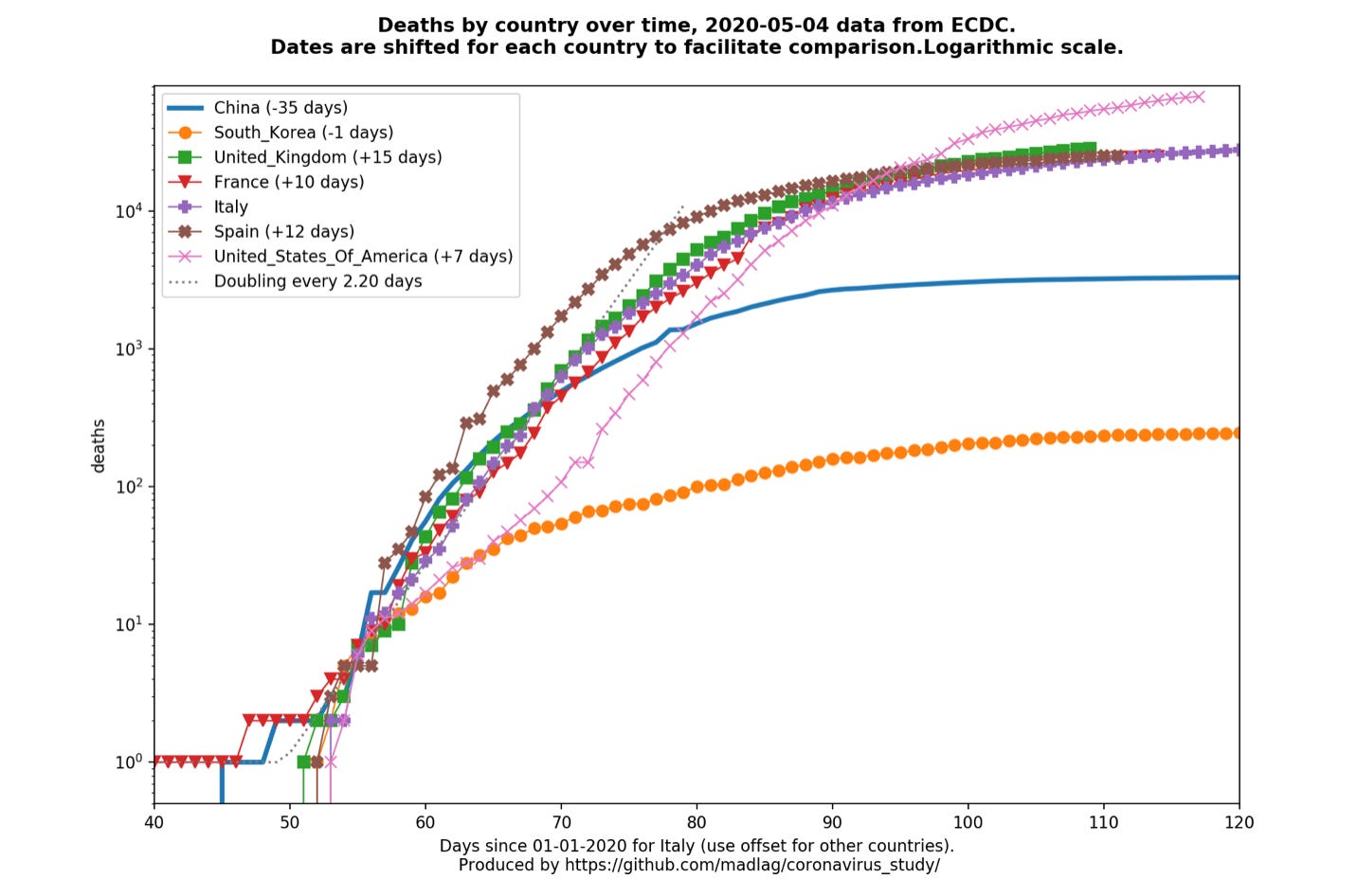
Death curves (updated daily as ECDC releases). Major update with per country graphs now available (Link) (US, UK, France, Germany, Sweden) (👈NEW❗️)
The toolbox gets better, research continues to progress, but complacency in re-opening remains a worry. Three of the themes covered in a short video and two twitter thread in this edition.
Ed Yong provides another great explainer on “mutations” and this controversial Bette Korber pre-print which was covered in yesterday’s Corona Daily (“Science at work”). Another explainer on physical (and potentially app-enabled) contact tracing which is key to successful re-opening and containment going forward.
It appears though from a survey in the Washington Post that people are still very weary of the virus and their habits and consumption will be affected. Re-opening or not the economy will continue to suffer as a result.
And then there is the likelihood of the African American people and business owners suffering most economically post re-opening. This is all the more disconcerting as this community also suffers more cases and fatalities from the virus.
NEW❗️I am open-sourcing my curated feeds and making them freely available below.
🦠 Video of the day: Another interesting interview of former FDA director Scott Gottlieb mentioning how the toolbox will get better (remdesivir, antibodies drug in the fall all in significant quantity, one or more vaccines to mass inoculate a population as part of a trial, and better testing) but still “the fall worries him a lot”. (Link)


🧪Thread of the day: Testing-Tracing-Isolating
Caitlin Rivers writes a thread about her testimony with the House Appropriations Subcommittee on Labor, HHS, & Education on the COVID-19 response. (First Tweet and Twitter thread)
Rivers, who has been stellar in her work and advice since the beginning of this pandemic, warned about complacency and the need to continue to build testing and tracing capacity:

If you have seen everything you wanted on Netflix you can watch the whole hearing here (2h 24min)
🧬 Article of the day: Ed Yong writes “The Problem With Stories About Dangerous Coronavirus Mutations” for the Atlantic. (Link)
This is a great follow-up article on the topic covered in yesterday’s Corona Daily (“Science at Work”) on the back of the controversial Bette Korber et al. pre-print paper on the D614G mutation.
Yong provides a great explainer about virus mutations and their significance or not. It also recounts the single amino-acid mutation (A82V - Alanine to Valine at position 82) in Ebola, and the responsible way it was published about then:
“Two independent teams of scientists showed that during the West African Ebola outbreak, that virus picked up a mutation called A82V, which made it better at infecting lab-grown human cells. Those teams had a stronger case than the Los Alamos team now does for SARS-CoV-2—but they still clarified that they didn’t know whether the mutation influenced the course of the historic outbreak. Sure enough, later work revealed that the A82V mutation doesn’t affect Ebola’s ability to infect actual animals.”
It also references Dr Angela Rasmussen Twitter thread which singled-out this Ebola precedent, and the careful way the scientists had reported on the discovery relative to the Los Alamos team.
I still believe that the sensational way the LA Times covered the pre-print, and the phrase “urgent need for an early warning” in its abstract, did a disservice to the work published by Bette Korber and her team.
On the positive side, it potentially gave the public an example of science and peer-review at work, which everybody can learn from including politicians who claim that they “follow the science”.
😰 Picture of the day: Dan Balz and Emily Guskin write “Americans widely oppose reopening most businesses, despite easing of restrictions in some states, Post-U. Md. poll finds.” As China initially discovered with its re-opening, re-opening manufacturing does not necessarily re-opens consumptions.
The article above focuses on the consumption without looking at the unease of retail workers whose employer will decide to re-open. A human factor seldom taken into account by early re-opening advocates. (Link)

🧪 Dylan Scott writes “Contact tracing, explained” in Vox. This is a good explainer on what contact tracing involves.
Scott also touches upon how contact tracing apps could help in spite of their known shortcomings, but mainly how human intensive the process is (including training):
“The Johns Hopkins Center for Health Security estimated the US needs 100,000 people performing this work for state and local agencies. Former Centers for Disease Control and Prevention Director Tom Frieden told Politico the necessary number of workers could be as high as 300,000.”
(Link)
🧪 Florian Krammer reports on a pre-print (not pee-reviewed) he and his team co-authored: “Humoral immune response and prolonged PCR positivity in a cohort of 1343 SARS-CoV 2 patients in the New York City region”.
“Here we show that the vast majority of confirmed COVID19 patients seroconvert, potentially providing immunity to reinfection. We also report that in a large proportion of individuals, viral genome can be detected via PCR in the upper respiratory tract for weeks post symptom resolution, but it is unclear if this signal represents infectious virus.”
As one of Krammer’s tweet in the thread says:

The pre-print also goes to give a potential explanation from these “reported re-infection”, as previously described in the video interview of World Health Organisation technical lead Dr Maria Van Kerkhove.
A positive thread and pre-print from a great group of scientists. (First Tweet and Twitter thread)
🛑 Aaron Ross Coleman writes “The near-certainty of a black depression” in Vox. The subtitle is even more telling: “Recessions are always racist. This one could be catastrophic.”
The Corona Daily previously reported on the inequality in case and fatality numbers affecting the African American community. Coleman takes us through the history of recessions in the US over the past century and how black communities have always been the hardest hit. It is likely that this one will even be worse. (Link)
🇺🇸 Tara C. Smith (Professor of Epidemiology at Kent State University in Ohio) writes “The Pandemic Will Soon Test Rural America” for Foreign Affairs:
Smith’s academic work focuses on disease transmission in rural areas. While urban communities (especially with New York accounting for a quarter of US fatalities) have been hardest hit by the pandemic, Smith worries about the spread of COVID-19 in rural America, she writes
“But rural areas are woefully unprepared for even a slower-moving epidemic. Just as they have suffered factory closures and job losses over the last decade, these regions have been devastated by the loss of hospitals and medical personnel. One hundred and twenty-eight rural hospitals have closed since 2010, scattered across the country but concentrated in the South and Midwest.”
An important warning. (Link)
📊 A picture is worth a thousand words: Global (🌎) and local (with relevant flag) visualisation and forecasting tool
🇺🇸
NEW❗️“Is your community ready to reopen?”: A map of the US (50 states and 2,100+ counties) looking at reopening risks with metrics around 3 criteria: 1. Is COVID in retreat? 2. Are we testing enough? 3. Are our hospitals ready? (Link)🌎The Financial Times (visualisation) has a data tracking page which is in front of the paywall, looking at cases and fatality curves for selective countries and metropolitan areas/region. It is not as extensive as the Madlag link below, where you can see static as well as animated images for a greater number of individual countries. (Link)🇺🇸 The John Hopkins University resource center was the first one I used back in January they have now made available in their latest iteration a county by county dashboard in the US including information about health capacity, insurance coverage, ethnicity and age breakdown of the population (New York example below) (Link)
💊 The "Map of Hope" provides a geographical overview of planned, ongoing and completed clinical trials. It is put together with data from WHO Clinical Trials Search Portal by the Heidelberg Institute for Geoinformation technology. (Link)
🌍 MRC Centre for Global Infectious Disease Analysis started to publish weekly death estimates for countries (Link)
🇺🇸 The US Center for Disease Control and Surveillance (CDC) publishes “A Weekly Surveillance Summary of U.S. COVID-19 Activity” (Link)
Google has published a new website to “See how your community is moving around differently due to COVID-19”. They have a lot of data to do so… (Link)
🌎 Country by Country Curves: This is a GitHub made by my friend Francois Lagunas. He has written a script to scrape deaths and number of cases in order to visualise the rate of growth on a logarithmic scale. Great resource (Link)
🌎A great resource put together by Ben Kuhn and Yuri Vishnevsky. At a time when we need solidarity and cooperation, I prefer their subtitle “We need stronger measures, much faster” than their title. It’s a simulator on what case growth looks like depending on your community’s measures. Fantastic resource to stir communities and governments to action (Link)
🇩🇪 The COVID19 dashboard for Germany is one of the best around. (Link)
🌎Data and chart regularly updated by the Centre for the Mathematical Modelling of Infectious Diseases at the London School of Hygiene & Tropical Medicine. It maps the effective reproduction number (also known as R0) of COVID19. You want to get it below 1 as fast as possible to contain an epidemic. (Link to see charts and more data about your country)