


🦠 COVID-19 | Once spiked twice shy?

I am a scientist by education, banker at JPMorgan for a few years, then mature PhD student in Chemical Biology at Oxford under the supervision of Christofer Schofield (FRS) and Peter Ratcliffe (Nobel laureate in medicine in 2019). Founder and tech investor focusing on media and education. I care about science, learning and Democracy which are good bedfellows.
📊 Daily Data Brief:
3,128,388 (+124,499) cumulative cases
Active cases: 1,960,493 (+46,384) (this is the number of currently infected patients)
Total Deaths: 217,017 (+9,914)
Serious/Critical Cases: 56,542 (-1,093)
Recovered: 950,878 (+68,201)
Source: Worldometers
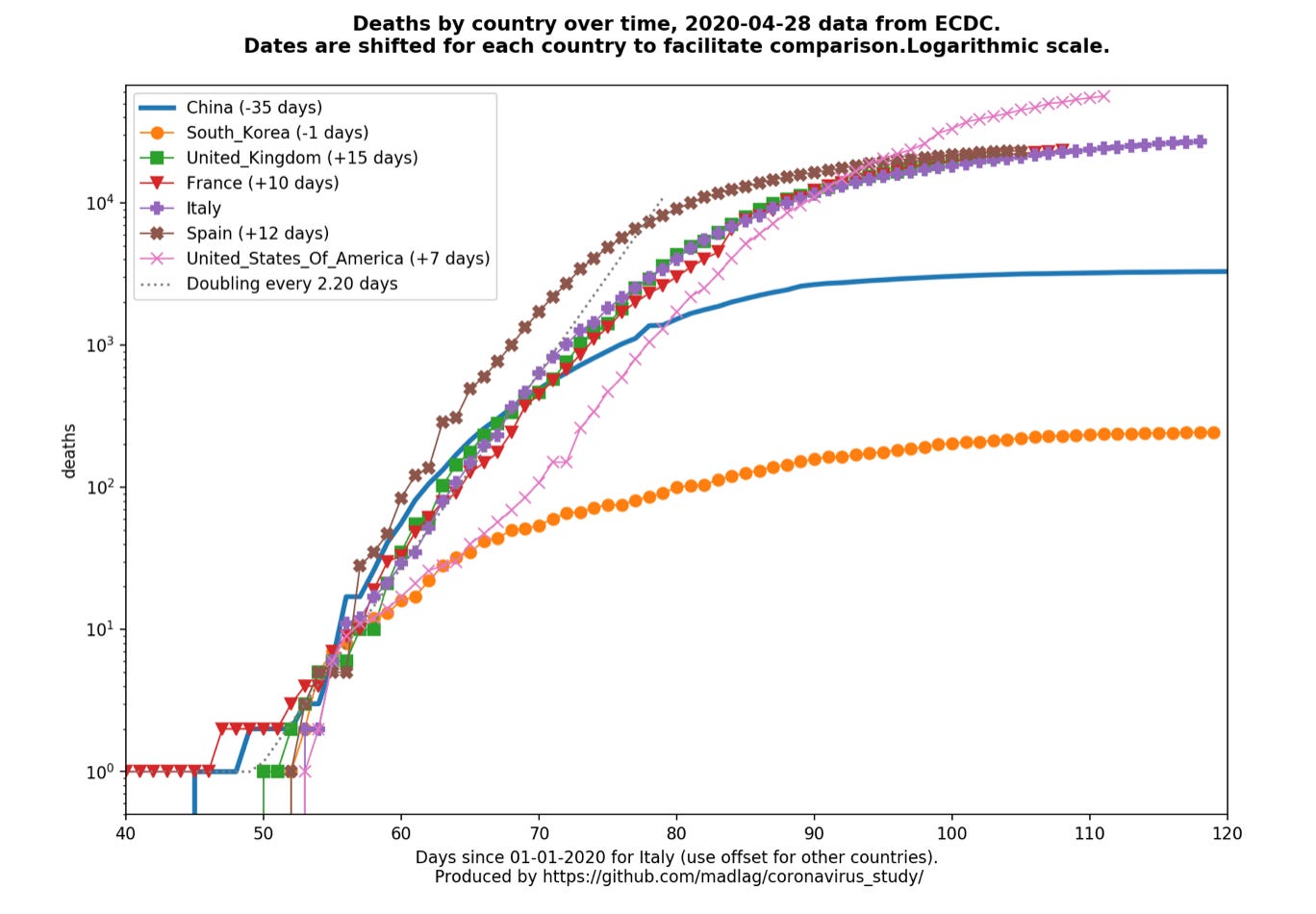
Death curves (updated daily as ECDC releases). Major update with per country graphs now available (Link) (US, UK, France, Germany, Sweden) (👈NEW❗️)
The spike protein in COVID19 is its key characteristics and the focus in most drug discovery and vaccine efforts against it. Vaccine is a large focus of the Corona Daily today with two great articles on whether we should run “Human challenge trials” and an explainer on the 8 different approaches being pursued in the race to a vaccine.
A great profile of the coronavirus tsar from Berlin, Christian Drosten, whose warning we did not heed mid January and which governments and states around the world seem to ignore again when it comes to re-opening. A reality check on testing ourselves out of the pandemic. A great in-depth article on how the US became dependent on China for 80% of its antibiotic supply. Finally, what can we learn from COVID19 to better address climate challenge ahead.
At the moment, it could be that we are heading for “One spiked, twice spiked” instead of “Once spiked twice shy”.
💉 Article of the day: Shayla Love writes “People Are Willing to Risk Their Lives for a COVID Vaccine. Should We Let Them?” for VICE. (Link)
This is an interview of Arthur Caplan, a bioethicist at New York University, who recently co-published with Stanley Plotkin “Extraordinary diseases require extraordinary solutions” in Vaccine journal advocating for human challenge trials for the COVID19 vaccine. Such trials consist in giving people an experimental vaccine and then deliberately infecting them to speed up the vaccine trial. In a regular trial people given the vaccine wait to be infected naturally thereby lengthening the trial duration.
I would recommend reading this article in conjunction with the one Jon Cohen wrote for Science titled: “Speed coronavirus vaccine testing by deliberately infecting volunteers? Not so fast, some scientists warn”. It is a good summary but also offers dissenting views from Caplan’s on the ethics of running human challenge trials. For example, Matthew Memoli, an immunologist at the U.S. National Institute of Allergy and Infectious Diseases who stages human challenge studies of influenza, worries about the large knowledge gaps we still have about COVID19 and argues against human challenge trials:
“Where you’re going to give somebody a virus on purpose, you really want to understand the disease so that you know that what you’re doing is a reasonable risk”
The interview is a fascinating journey to the ethics and design of human challenge trials for COVID19 vaccine candidates, particularly at a time when a grassroot organisation called 1 Day Sooner has already had 3,900 volunteers signup for such trials.
In the middle of the interview Caplan makes an important distinction:
“We’re not calling for no consent or no review. We’re not calling to abandon the ethics that have governed research. I don’t think we should run around deliberately injecting people. You wouldn't want to do these studies in poor nations where they might be exploited. But it’s wrong to think that we’ve never done the challenge study work that we have.”
Caplan believes that the conditions are there to proceed with human challenge trials for vaccine candidates with the highest standard in terms of consent and design of the trials. He ends up with a quote which will resonate with many:
“There is another situation here which is that, while we're bemoaning stretching the research in trying to get a fast answer to various antiviral drugs that are rattling around, we at the same time allow the president to stand up for two hours every day and direct absolute nonsense at the population with no one standing there to correct his risk and benefit calculations. Instead we try to interpret if Tony Fauci is grimacing or Dr. Birx is frowning. In a society that is willing to tolerate letting people poison themselves because they're afraid to take on the president, arguing about a challenge study seems a bit of a luxury.”
Tweet of the day: A follow up to yesterday’s Corona Daily (“Failing the Marshmallow test”). Wuhan lifted its lockdown after 76 days. US States and European countries are lifting or planning to lift their lockdown after fewer days: are they eating their marshmallow?


💉 Ewen Callaway writes “The race for coronavirus vaccines: a graphical guide” for Nature. This is a great explainer of how one develops immunity and the 8 different types of vaccine approaches being tried to develop a vaccine. All you ever wanted to know about vaccines. (Link)
🧪 Michael T. Osterholm (director of the Center for Infectious Disease Research and Policy at the University of Minnesota) and Mark Olshaker write “Let’s Get Real About Coronavirus Tests” for the New York Times. Since the beginning of the pandemic there has been a lot of focus on testing, from the initial fiasco in the US, to the continued under-availability of testing in most countries, to advocating testing being our way out of the crisis and the key to returning to a new normal.
The author somewhat pour cold water on the reality on the ground of the last claim, not challenging its possibility, but arguing instead that we are not able given both quantity and quality of testing available to perform effectively a testing-tracing-isolate strategy out of the crisis. Our initial focus on quantity of testing meant that not only quality has suffered but also that reagents to scale production of these tests have been in short supply.
When it comes to diagnostic tests (performed with RT-PCR), rate of ‘false negatives’ remains problematically high, risking to leave infected citizens to freely roam and infect others. When it comes to serological testing and as the Corona Daily has reported in previous editions there remains unknowns as to what to make of a positive anti-body test:
These features are one reason an April 17 advisory from the F.D.A.recommending the use of serological tests simultaneously warned that the agency “does not expect that an antibody test can be shown to definitively diagnose or exclude SARS-CoV-2 infection.” Last Friday, the World Health Organization released a scientific brief that said, “There is currently no evidence that people who have recovered from Covid-19 and have antibodies are protected from a second infection.”
What do the authors suggest until tests’ quality and quantity get better? Scale “syndromic surveillance” which consists in tracking patients with symptoms associated with COVID19. (Link)
👨⚕️ Kai Kupferschmidt “How the pandemic made this virologist an unlikely cult figure” for Science. We featured an interview in the Guardian of Christian Drosten (director of the Institute of Virology at the Charité Hospital in Berlin) in Sunday’s Corona Daily. Dorsten has tracked coronaviruses since 2003:


Kupferschmidt narrates how Drosten came to develop the first test for SARS whilst still a PhD student back in 2003 and how he continued his career focusing on coronaviruses, repeated the feat with his lab developing and publishing the first test for SARS-CoV2 mid-January (!). He now takes part in a twice-weekly podcast on the pandemic downloaded by over 1 million people.
The article recounts on how Drosten was growing exasperated when doing interviews in January:
Drosten started to warn of the new virus’ potential in TV interviews in January, but quickly grew exasperated. After long interviews, journalists often used one short quote that failed to convey the immense threat, he says. “I actually called up some of them afterwards and told them: ‘You are missing the boat on this.’”
This part poses serious questions about why this exasperation at the time was not taken seriously not only by the TV journalists but the rest of the world, and how going forward we need to revaluate the relationship between science, policy and the public.
His most recent exasperation is about the disproportionate impact (from a political point of view) given to a not-peer reviewed serological study in one small town in Germany. The study implied a lower fatality rate for SARS-CoV2 than widely believed and higher prevalence in the population. This was a strong political catalyst for the opening underway in Germany:
“That concern has led him to depart from his science-only strategy. “In this situation, for once, I have to express my opinion a little bit here in this podcast,” he said on 22 April. Discussing press reports of shopping malls full of people, he said, “It’s sad to see that we may be in the process here in Germany of completely gambling away the advantage we have had.”
The world seems not to have heeded Dorsten words mid-January and seems now to do the same with reopening. (Link)
❗️ Gardiner Harris and Alex W. Palmer write “China has near-total control of the world’s antibiotic supply. Is America at risk as a result?” for STAT+. This article dissects the following critical issue:
“The country where the novel coronavirus originated makes 80% of all antibiotics, humanity’s primary weapon against bacterial infection.”
How did we let this happen? Was it the neglect of public health, incompetence, recklessness or an obsessive and blind focus on profit from big pharma (particularly post the arrival of generic drugs in 1984). Or was it also the convenient export of pollution to China:
“Then there were the costs of environmental oversight. Antibiotics production creates an enormous amount of dirty water that must be cleaned before it is discharged. Making a single kilogram of penicillin can produce 10 tons of effluent.”
In 2019, Rosemary Gibbons (author of “China Rx: Exposing the Risks of America's Dependence on China for Medicine” ) warned eloquently a Capitol Hill Committee about the risk:
“If China shut the door on exports of medicines and their key ingredients and raw materials, U.S. hospitals and military hospitals and clinics would cease to function within months, if not days. A natural disaster, global public health crisis or adverse foreign government action could disrupt the supply of medicinal ingredients and finished drugs. Medicines in the hands of an adversary can be weaponized”
The COVID19 pandemic have made shortages risk a reality 49 new drug shortages in 2020 alone. In spite of all these well established risks, it remains a doubt whether antibiotics will come back to the US, for the same reasons (cost and pollution) they left in the first place. Chilling. (Link)
🌍 “What can firms' COVID-19 strategies teach us about the climate battle ahead” for the World Economic Forum.
“Changes to the way businesses are operating due to COVID-19 are reducing carbon emissions.
Rethinking supply chains could lead to a sustained drop in transport-related emissions.
Governments can use stimulus packages to bake-in commitments to more sustainable business practices in future.”
Interesting read and rational expectation. Emergency politics and a short exit of the crisis could make these more wishful thinking than a new reality. (Link)
🎬 🦘 “Animals reclaiming the world” video (Link)


📊 A picture is worth a thousand words: Global (🌎) and local (with relevant flag) visualisation and forecasting tool
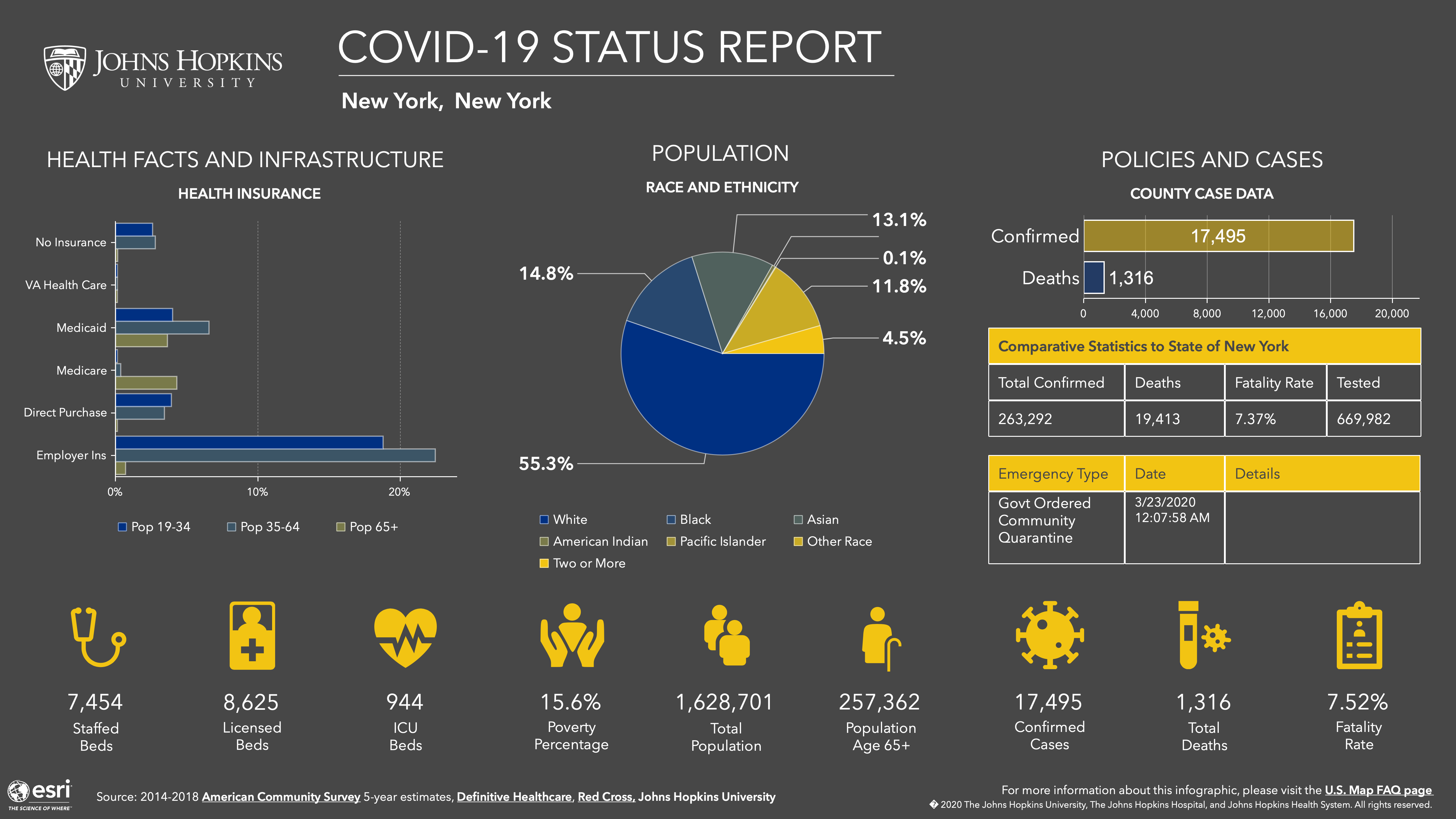
🌎The Financial Times (NEW❗️visualisation) has a data tracking page which is in front of the paywall, looking at cases and fatality curves for selective countries and metropolitan areas/region. It is not as extensive as the Madlag link below, where you can see static as well as animated images for a greater number of individual countries. (Link)🇺🇸 The John Hopkins University resource center was the first one I used back in January they have now made available in their latest iteration a county by county dashboard in the US including information about health capacity, insurance coverage, ethnicity and age breakdown of the population (New York example below) (Link)
💊 The "Map of Hope" provides a geographical overview of planned, ongoing and completed clinical trials. It is put together with data from WHO Clinical Trials Search Portal by the Heidelberg Institute for Geoinformation technology. (Link)
🌍 MRC Centre for Global Infectious Disease Analysis started to publish weekly death estimates for countries (Link)
🇺🇸 The US Center for Disease Control and Surveillance (CDC) publishes “A Weekly Surveillance Summary of U.S. COVID-19 Activity” (Link)
Google has published a new website to “See how your community is moving around differently due to COVID-19”. They have a lot of data to do so… (Link)
🇺🇸Another valuable resource by Unacast ( a data company providing human mobility insights). Their “Social distancing scoreboard looks and compares (State by State and County by County), the change in mobility to prior to COVID19 (Link)
🌎 Country by Country Curves: This is a GitHub made by my friend Francois Lagunas. He has written a script to scrape deaths and number of cases in order to visualise the rate of growth on a logarithmic scale. Great resource (Link)
CityMapper has started to produce City Mobility Index to show how much a City is moving. This is a very good indicator of how well lockdowns are respected around the world: Barcelona (4% of city moving) at one end and St Petersburg at the other end (68% of city moving) for yesterday (Link)
🌎A great resource put together by Ben Kuhn and Yuri Vishnevsky. At a time when we need solidarity and cooperation, I prefer their subtitle “We need stronger measures, much faster” than their title. It’s a simulator on what case growth looks like depending on your community’s measures. Fantastic resource to stir communities and governments to action (Link)
🇩🇪 The COVID19 dashboard for Germany is one of the best around. (Link)
🌎Data and chart regularly updated by the Centre for the Mathematical Modelling of Infectious Diseases at the London School of Hygiene & Tropical Medicine. It maps the effective reproduction number (also known as R0) of COVID19. You want to get it below 1 as fast as possible to contain an epidemic. (Link to see charts and more data about your country)
🌎This is a great COVID19 Dashboard prepared by Andrzej Leszkiewicz. Andrzej has also written an introductory and explanatory blog for it (“Coronavirus disease (COVID-19) fatality rate: WHO and media vs logic and mathematics”). I particularly like the country comparison tab, which allows you to track and benchmark the curve of the epidemic (number of cases and deaths) in your country with that of another. Very well done and informative. (Link)
🏛 Notable tracking projects
💊“COVID-19 treatment and vaccine tracker”. This tracker contains an aggregation of publicly-available information from validated sourcesby the Milken Institute (Link)🏛Tariq Krim has started a COVID19 website tracking data about each government policy response to the pandemic (Link)
🏛Oxford COVID-19 Government Response Tracker (OxCGRT) was launched yesterday. Data is collected from public sources by a team of dozens of Oxford University students and staff from every part of the world. It also looks at stringency of the measures and plots stringency with case curves. A great initiative and resource (Link)
📰 Cronycle resource:
Cronycle has made available a number of open-access feeds on its website which I extensively use for the Corona Daily. The four first feeds are:
1. COVID-19 General (Link)
2. COVID-19 x Resilience (Link)
3. COVID-19 x HCQ/CQ (Link) (HydroxyChloroquine and Chloroquine)
4. Gig Economy x COVID-19 (Link) 5. Supply Chain x COVID-19 (Link)
5. Supply Chain x COVID-19 (Link)
Human Rights x COVID-19 (Link)